Comparative effectiveness and personalized medicine research using real-world data
Background

IMI GetReal: Incorporating real-life clinical data into drug development
- GetReal aimed to show how robust new methods of real-world evidence collection and synthesis could be adopted earlier in pharmaceutical research and development and the healthcare decision-making process.
- Together with Bern, we investigated statistical methods for network meta-analysis
ISCB Utrecht

The Hierarchy of Evidence Pyramid
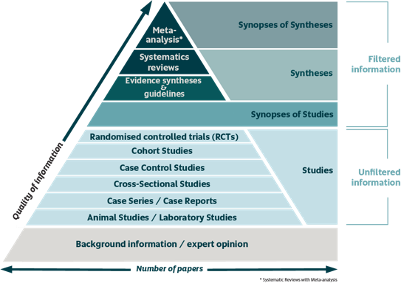
Limitations of randomized trials

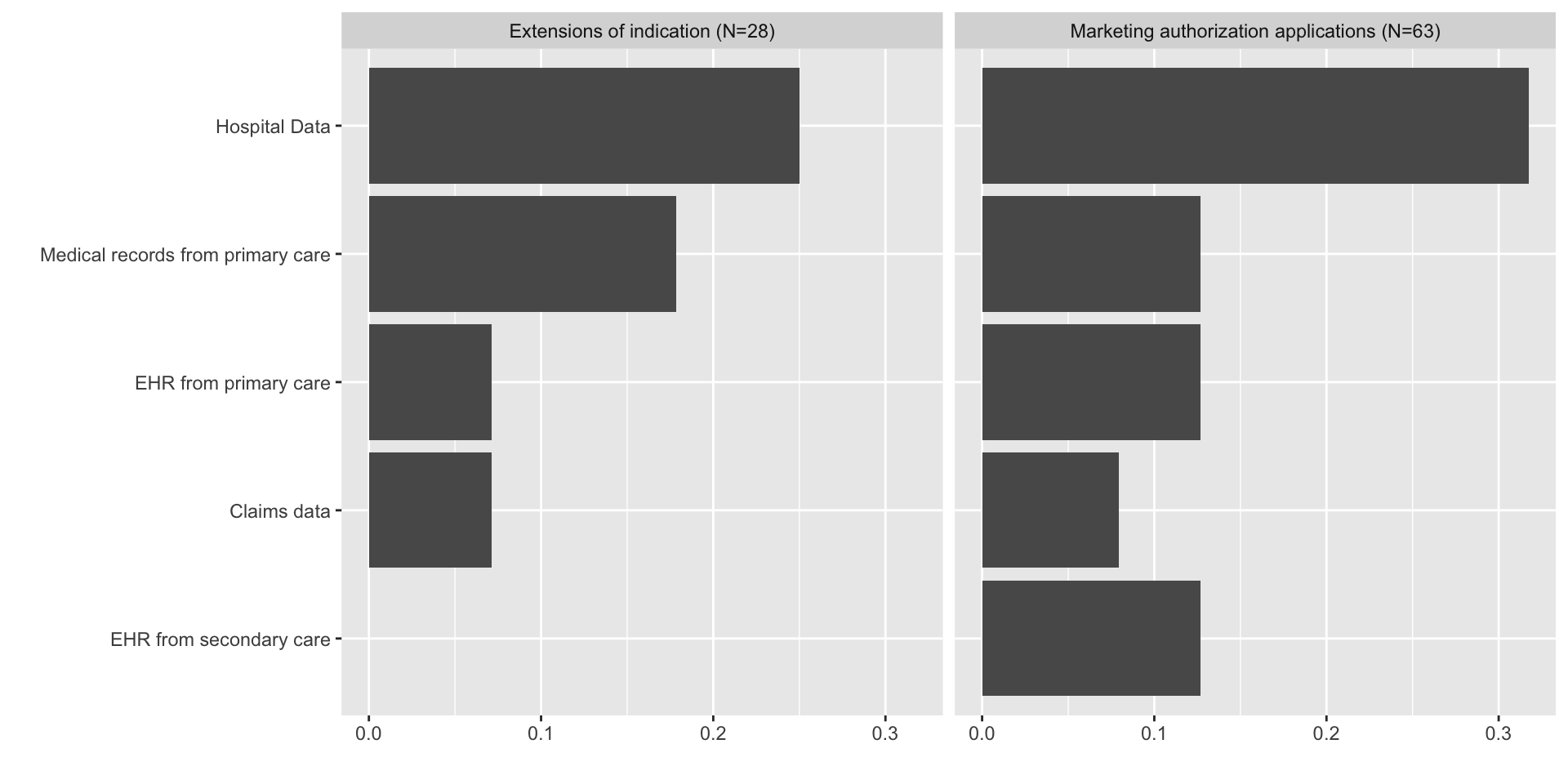
What is real-world data (RWD)?

Data relating to patient health status and/or the delivery of health care routinely collected from a variety of sources

Routinely collected data relating to a patient’s health status or the delivery of health care from a variety of sources other than traditional clinical trials

Data collected outside the context of a highly controlled clinical trial
What is real-world evidence (RWE)?
Evidence generated from the analysis of real-world data
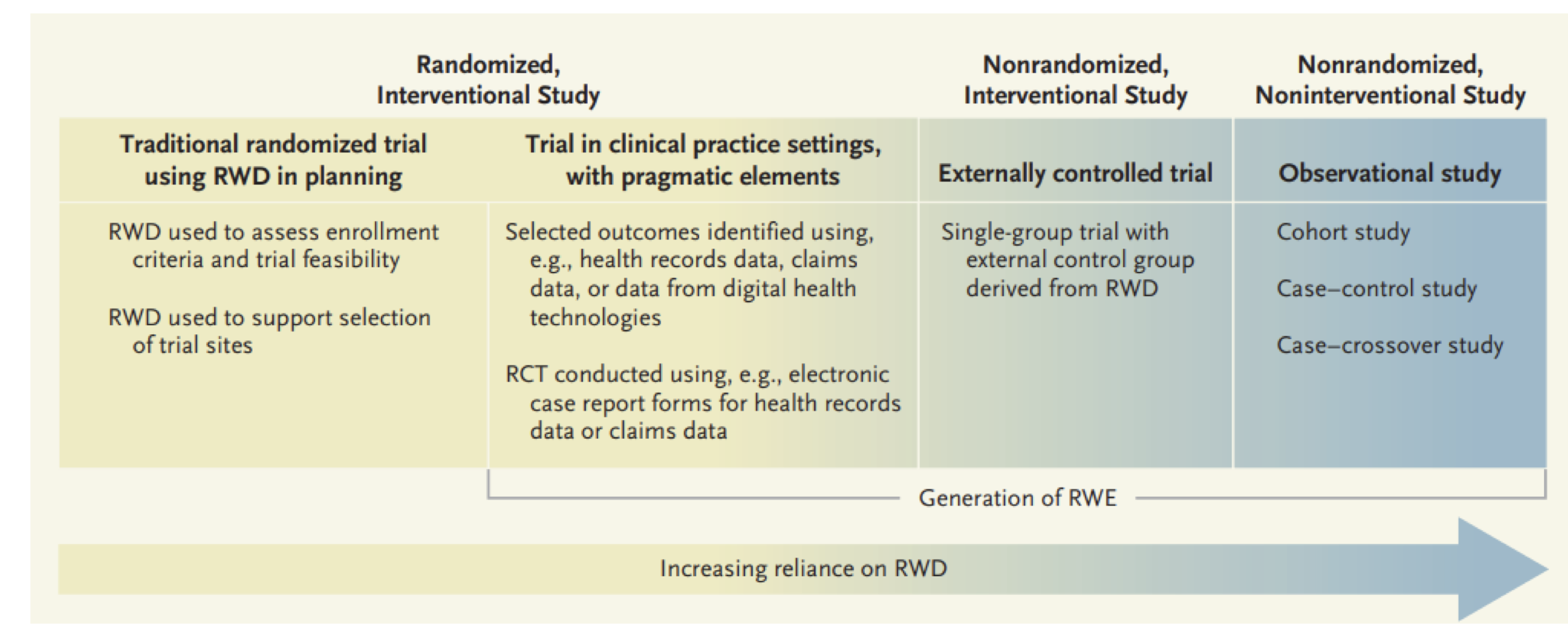
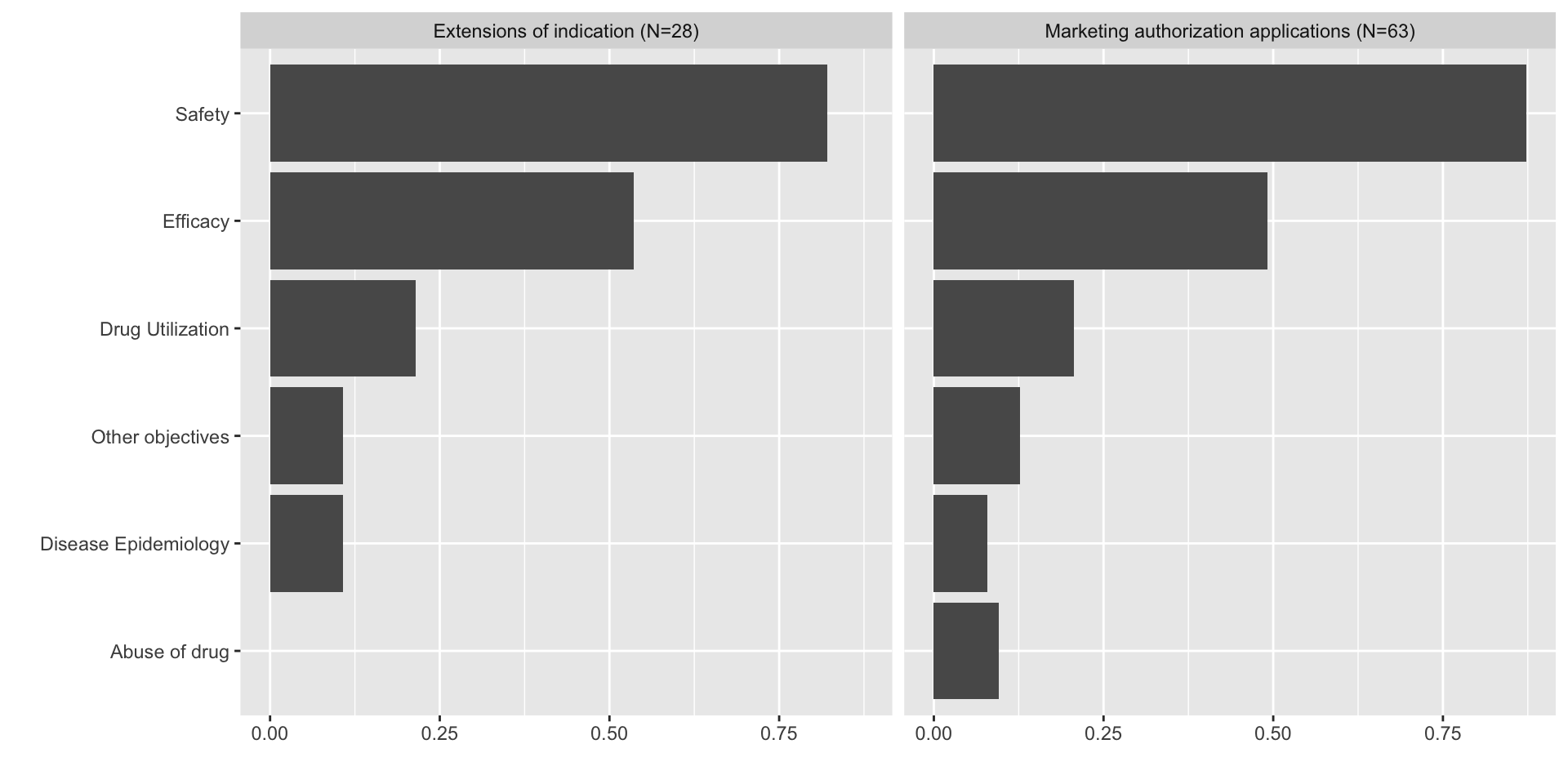
How is RWE used?
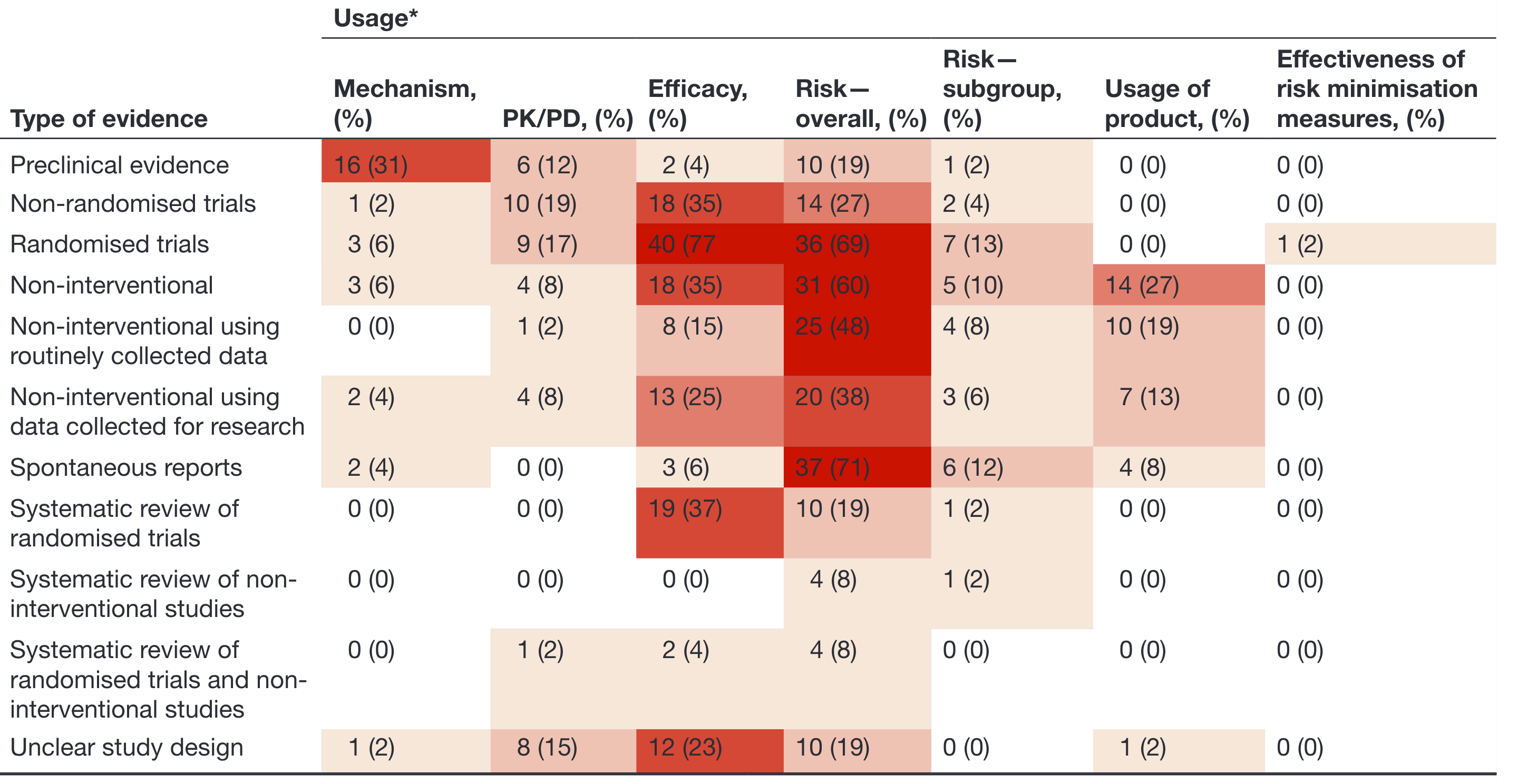
How is RWE used?
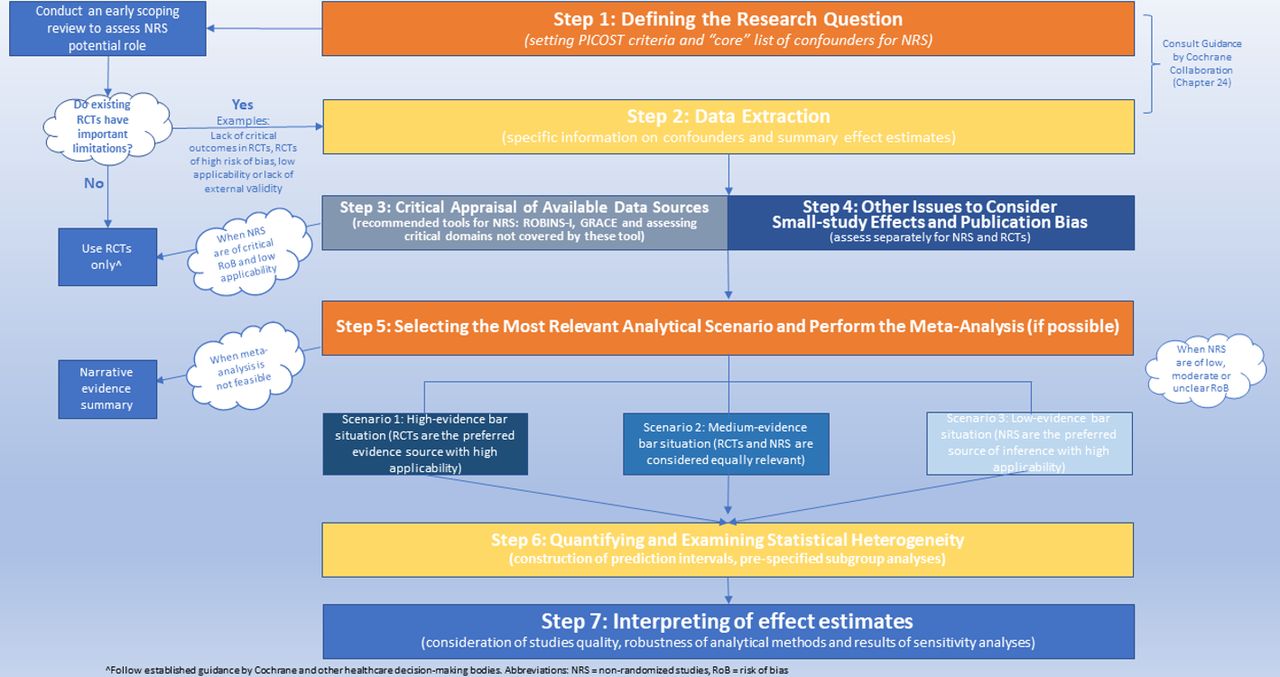
Recommendations for RWE studies
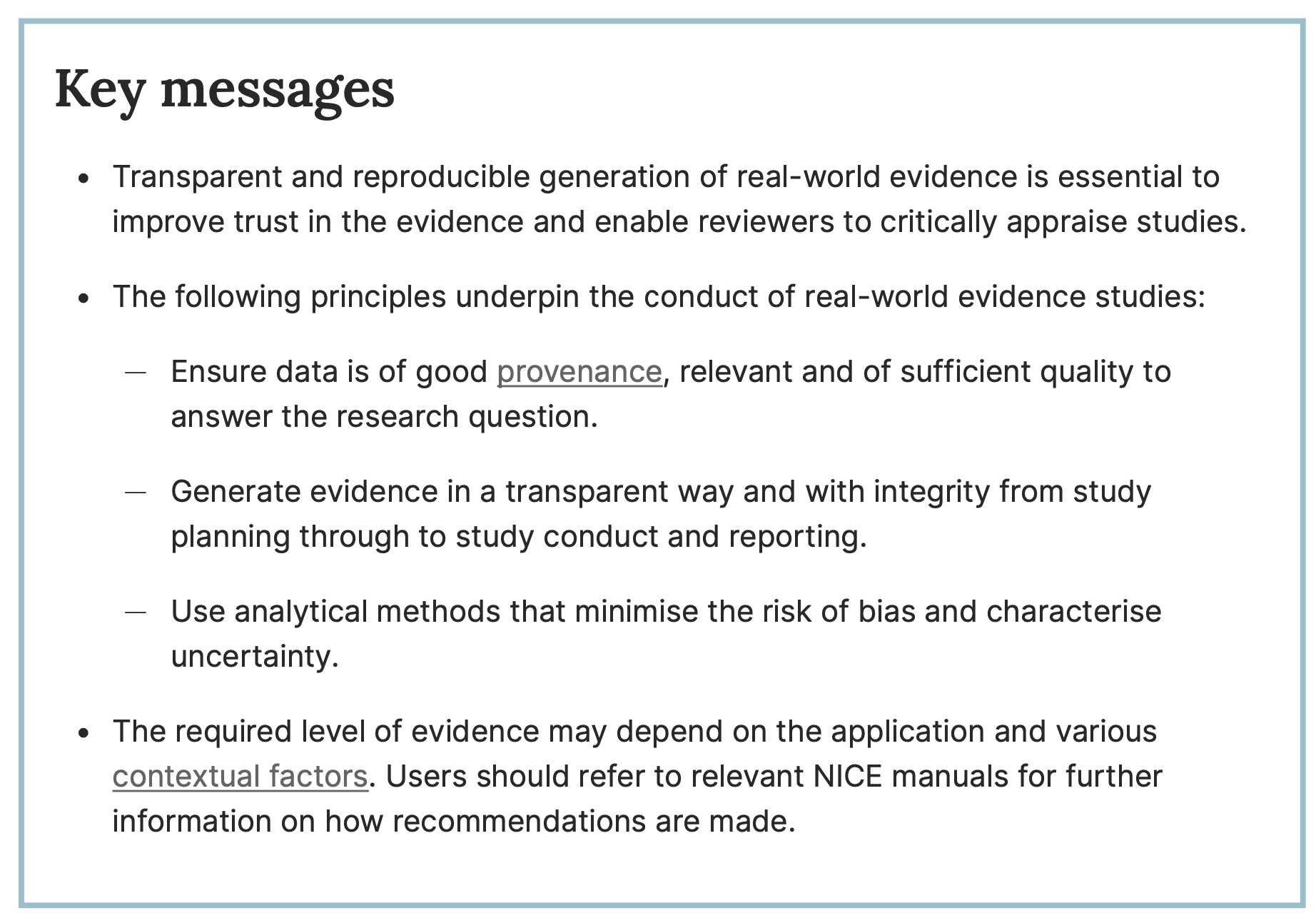
Recommendations for RWE studies
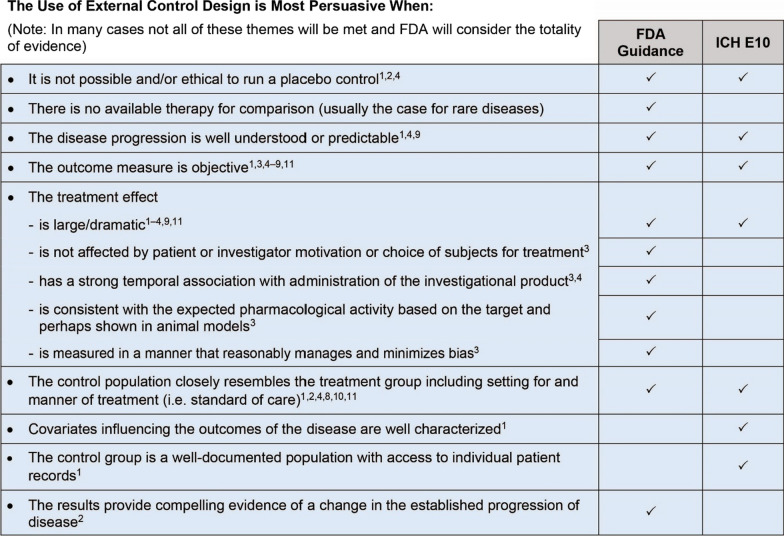
Recommendations for RWE studies
Regulatory decision making
- The future is not about randomized controlled trials (RCTs) vs. real-world evidence (RWE) but about RCTs and RWE — not just for the assessment of safety but also of effectiveness
- Patients will need to be followed up for prolonged periods of time to empirically confirm or refute a priori comparative effectiveness assumptions
Data platforms
![]()
Catalogue of observational data sources for use in medicines regulation
![]()
Federated data network of allowing access to the data of EU citizens standardised to a common data model.
Estimating individualized treatment effects
precmed: Precision Medicine
A doubly robust precision medicine approach to fit, cross-validate and visualize prediction models for the conditional average treatment effect. Available from GitHub and CRAN.
Comparative effectiveness and personalized medicine using real-world data
- Edited by TPA Debray, T-L Nguyen and RW Platt
- 21 chapters; publication expected in 2024
- Contributions from ~ 40 authors (academia; industry; contract resesarch organizations; health technology assessment agencies; regulatory decision-making)
- Example code on GitHub

